Do I Have Fallen Arches??
Overview

When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Causes
Abnormal development of the foot, producing Pes Planus, may be due to neurological problems, eg cerebral palsy, polio. Bony or ligamentous abnormalities, eg tarsal coalition (fusion of tarsal bones), accessory navicular bone. A small proportion of flexible flat feet do not correct with growth. Some of these may become rigid if the Pes Planus leads to bony changes.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
arch support for flat feet
Non Surgical Treatment
When pain results from a fallen arch, the physician may prescribe these. Rest and ice. A brace to help support the fallen arch. Physical therapy to strengthen and stretch the foot. Orthotics (arch supports) to compensate for a fallen arch. The physician may tell the patient to choose shoes that have proper arch supports and avoid non-supportive shoes such as flip-flops. If obesity contributed to the fallen arch, the patient should lose weight.
Surgical Treatment

A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery.
When sitting, an over-pronating foot appears quite normal, i.e. showing a normal arch with room under the underside of the foot. The moment you get up and put weight on your feet the situation changes: the arches lower and the ankle slightly turns inwards. When you walk or run more weight is placed on the feet compared to standing and over-pronation will become more evident. When walking barefoot on tiles or timber floors over-pronation is more visible, compared to walking on carpet or grass.
Causes
Abnormal development of the foot, producing Pes Planus, may be due to neurological problems, eg cerebral palsy, polio. Bony or ligamentous abnormalities, eg tarsal coalition (fusion of tarsal bones), accessory navicular bone. A small proportion of flexible flat feet do not correct with growth. Some of these may become rigid if the Pes Planus leads to bony changes.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
If your child has flatfeet, his or her doctor will ask about any family history of flatfeet or inherited foot problems. In a person of any age, the doctor will ask about occupational and recreational activities, previous foot trauma or foot surgery and the type of shoes worn. The doctor will examine your shoes to check for signs of excessive wear. Worn shoes often provide valuable clues to gait problems and poor bone alignment. The doctor will ask you to walk barefoot to evaluate the arches of the feet, to check for out-toeing and to look for other signs of poor foot mechanics. The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma.
arch support for flat feet
Non Surgical Treatment
When pain results from a fallen arch, the physician may prescribe these. Rest and ice. A brace to help support the fallen arch. Physical therapy to strengthen and stretch the foot. Orthotics (arch supports) to compensate for a fallen arch. The physician may tell the patient to choose shoes that have proper arch supports and avoid non-supportive shoes such as flip-flops. If obesity contributed to the fallen arch, the patient should lose weight.
Surgical Treatment
A combination of surgical procedures can be used to reconstruct the flatfoot. Generally, these procedures can be separated into those that correct deformities of the bones and those that repair ligaments and tendons. Your orthopaedic surgeon will choose the proper combination of procedures for your foot. Surgery of the foot can be performed under regional anesthesia, which is numbing the foot and ankle with a nerve or spinal block, or general anesthesia, which may require a breathing tube. A nerve block is often placed behind the knee to reduce pain after surgery.
Heel Aches The Causes, Signs And Symptoms And Treatment Methods
Overview

The heel is a padded cushion of fatty tissue around the heel bone (the calcaneus) that holds its shape despite the pressure of body weight and movement. It serves to protect the structures of the foot, including the calcaneus, muscles and ligaments. Heel pain is a very common foot complaint. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including Middle-aged men and women, Physically active people, People who are overweight or obese, People who are on their feet for long periods of time, Children aged between eight and 13 years (particularly boys), Women during pregnancy.
Causes
The most common local causes of heel pain include. Plantar fasciitis, plantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur, a heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, in this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump, this condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Like other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. In most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Compression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Sever?s Disease. This is a condition that occurs in 10 - 15 year old children, predominantly boys and is associated with running and repetitive jumping. It is also associated with flimsy footwear that kids may wear. It occurs when the Achilles tendon continually pulls on the apophysis of the calcaneum and does not allow for it to fuse with the body of the calcaneum. Calcaneal enthesopathy. This occurs when there is repetitive trauma at the attachment of the Achilles tendon, resulting in a spur from the calcaneum up into the Achilles tendon. It is usually visualized on x-ray and may be tender if there is an associated bursitis or tendonitis. "Pump Bump". Also known as Haglund?s Deformity, this is a bony enlargement that exists on the back of the heel - usually related to a congenital abnormality or with chronic bursitis, causing a thickening. There may have already been trauma or pressure from footwear. Treatment is usually protection of the bump and correct footwear. Associated with a symmetrical swelling at the base of the Achilles tendon. It is usually related to repetitive trauma or inappropriate footwear. It is often red and hot in the early stages. Treatment is usually to correct the footwear, provide padding and treat the local symptoms e.g. ice, rest, physiotherapy and cortisone injection. Fat Pad Syndrome. Direct contact with the base of the heel may result in trauma to the fat pad. Related to obesity, training on hard surfaces, uneven grounds, poor shoes especially overlarge shoes which can cause shearing forces on the heel. These conditions are renowned for taking a long time to recover - usually many months.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Rest until there is no more pain. This is the most important element of treatment as continuing to walk or run on the injured foot will not allow the injury to heal. Wear soft trainers with lots of cushioning or pad the heel of shoes with shock absorbing insoles or heel pads. These should be worn in both shoes, even if only one heel is bruised. Wearing a raise in only one shoe causes a leg length difference which can cause other problems. Replace running shoes if they are old. A running shoe is designed to last for around 400 miles of running. After this the mid soles are weakened through use.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
how to get rid of heel spurs
Prevention

Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
The heel is a padded cushion of fatty tissue around the heel bone (the calcaneus) that holds its shape despite the pressure of body weight and movement. It serves to protect the structures of the foot, including the calcaneus, muscles and ligaments. Heel pain is a very common foot complaint. Anyone can suffer from heel pain, but certain groups seem to be at increased risk, including Middle-aged men and women, Physically active people, People who are overweight or obese, People who are on their feet for long periods of time, Children aged between eight and 13 years (particularly boys), Women during pregnancy.
Causes
The most common local causes of heel pain include. Plantar fasciitis, plantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur, a heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, in this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump, this condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Like other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. In most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Compression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Sever?s Disease. This is a condition that occurs in 10 - 15 year old children, predominantly boys and is associated with running and repetitive jumping. It is also associated with flimsy footwear that kids may wear. It occurs when the Achilles tendon continually pulls on the apophysis of the calcaneum and does not allow for it to fuse with the body of the calcaneum. Calcaneal enthesopathy. This occurs when there is repetitive trauma at the attachment of the Achilles tendon, resulting in a spur from the calcaneum up into the Achilles tendon. It is usually visualized on x-ray and may be tender if there is an associated bursitis or tendonitis. "Pump Bump". Also known as Haglund?s Deformity, this is a bony enlargement that exists on the back of the heel - usually related to a congenital abnormality or with chronic bursitis, causing a thickening. There may have already been trauma or pressure from footwear. Treatment is usually protection of the bump and correct footwear. Associated with a symmetrical swelling at the base of the Achilles tendon. It is usually related to repetitive trauma or inappropriate footwear. It is often red and hot in the early stages. Treatment is usually to correct the footwear, provide padding and treat the local symptoms e.g. ice, rest, physiotherapy and cortisone injection. Fat Pad Syndrome. Direct contact with the base of the heel may result in trauma to the fat pad. Related to obesity, training on hard surfaces, uneven grounds, poor shoes especially overlarge shoes which can cause shearing forces on the heel. These conditions are renowned for taking a long time to recover - usually many months.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Rest until there is no more pain. This is the most important element of treatment as continuing to walk or run on the injured foot will not allow the injury to heal. Wear soft trainers with lots of cushioning or pad the heel of shoes with shock absorbing insoles or heel pads. These should be worn in both shoes, even if only one heel is bruised. Wearing a raise in only one shoe causes a leg length difference which can cause other problems. Replace running shoes if they are old. A running shoe is designed to last for around 400 miles of running. After this the mid soles are weakened through use.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
how to get rid of heel spurs
Prevention
Flexibility is key when it comes to staving off the pain associated with these heel conditions. The body is designed to work in harmony, so stretching shouldn?t be concentrated solely on the foot itself. The sympathetic tendons and muscles that move the foot should also be stretched and gently exercised to ensure the best results for your heel stretches. Take the time to stretch thighs, calves and ankles to encourage healthy blood flow and relaxed muscle tension that will keep pain to a minimum. If ice is recommended by a doctor, try freezing a half bottle of water and slowly rolling your bare foot back and forth over it for as long as is comfortable. The use of elastic or canvas straps to facilitate stretching of an extended leg can also be helpful when stretching without an assistant handy. Once cleared by a doctor, a daily regimen of over-the-counter anti-inflammatory medication like Naproxen Sodium will keep pain at bay and increase flexibility in those afflicted by heel pain. While this medication is not intended to act as a substitute for medical assessments, orthopedics or stretching, it can nonetheless be helpful in keeping discomfort muted enough to enjoy daily life. When taking any medication for your heel pain, be sure to follow directions regarding food and drink, and ask your pharmacist about possible interactions with existing medications or frequent activities.
Functional Leg Length Discrepancy Stretches
Overview
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).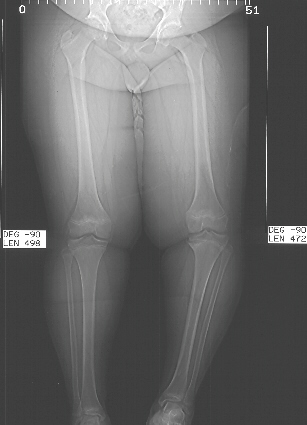
Causes
Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified.
Non Surgical Treatment
The way in which we would treat a LLD would depend on whether we have an anatomical or functional difference. To determine which one is causing the LLD you will need to get your legs measured. This is the easiest way to determine if it is anatomical or functional. With a functional LLD we must first determine the cause and treat the cause. Should the cause be one that is not correctable then we may need to treat the LLD as if it were an anatomical or may have to treat the opposite leg to improve one's gait. As for the anatomical LLD, we may start off with a heel lift only in the shoe and follow up to see if we will need to put the lift full sole on the bottom of the shoe. This is determined by the affects that a heel lift in one shoe may have on that knee. Should the LLD be more than 1/4 inch we usually recommend starting between 1/8 inch to 1/4 inch less than the actual amount and let the body adjust to the change and then raise up to the measured amount later.

how do you get taller in a day?
Surgical Treatment
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Causes
Some limb-length differences are caused by actual anatomic differences from one side to the other (referred to as structural causes). The femur is longer (or shorter) or the cartilage between the femur and tibia is thicker (or thinner) on one side. There could be actual deformities in one femur or hip joint contributing to leg length differences from side to side. Even a small structural difference can amount to significant changes in the anatomy of the limb. A past history of leg fracture, developmental hip dysplasia, slipped capital femoral epiphysis (SCFE), short neck of the femur, or coxa vara can also lead to placement of the femoral head in the hip socket that is offset. The end-result can be a limb-length difference and early degenerative arthritis of the hip.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
The evaluation of leg length discrepancy typically involves sequential x-rays to measure the exact discrepancy, while following its progression. In addition, an x-ray of the wrist allows us to more carefully age your child. Skeletal age and chronological age do not necessarily equal each other and frequently a child's bone age will be significantly different than his or her stated age. Your child's physician can establish a treatment plan once all the facts are known: the bone age, the exact amount of discrepancy, and the cause, if it can be identified.
Non Surgical Treatment
The way in which we would treat a LLD would depend on whether we have an anatomical or functional difference. To determine which one is causing the LLD you will need to get your legs measured. This is the easiest way to determine if it is anatomical or functional. With a functional LLD we must first determine the cause and treat the cause. Should the cause be one that is not correctable then we may need to treat the LLD as if it were an anatomical or may have to treat the opposite leg to improve one's gait. As for the anatomical LLD, we may start off with a heel lift only in the shoe and follow up to see if we will need to put the lift full sole on the bottom of the shoe. This is determined by the affects that a heel lift in one shoe may have on that knee. Should the LLD be more than 1/4 inch we usually recommend starting between 1/8 inch to 1/4 inch less than the actual amount and let the body adjust to the change and then raise up to the measured amount later.
how do you get taller in a day?
Surgical Treatment
Large leg length inequalities can be treated by staged lengthenings or by simultaneous ipsilateral femoral and tibial lengthenings. Additionally, lengthenings can be combined with appropriately timed epiphysiodesis in an effort to produce leg length equality. Staged lengthenings are often used for congenital deficiencies such as fibular hemimelia, in which 15 cm or more may be needed to produce leg length equality. We typically plan for the final lengthening to be completed by age 13 or 14 years, and allow at least 3 years between lengthenings. Lengthening of both the tibia and femur simultaneously requires aggressive therapy and treatment of soft tissue contractures. Curran et al[57] reported the need for surgical release of soft tissue contractures in 3 of 8 patients treated with simultaneous ipsilateral femoral and tibial lengthenings. Lengthening over an IM nail can be done in an effort to decrease the amount of time the fixator needs to be worn and to prevent angular malalignment. This technique requires that the patient be skeletally mature and it carries a higher risk of osteomyelitis (up to 15%). Additionally, if premature consolidation occurs, a repeat corticotomy is more difficult.
Mortons Neuroma Causes
Overview
 Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.
Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.
Causes
In many cases, a neuroma may develop as a result of excessive loading on the front of the foot. Sometimes, a patient?s anatomic alignment in the forefoot contributes to the overload. There may be some cases where the neuroma develops spontaneously, for no obvious reason. However, once the nerve is irritated, pressure from walking, and from the adjacent bony prominences (metatarsal heads), as well as from the intermetatarsal ligament that binds the heads together, all may contribute to persistent pain. Repetitive pressure on the nerve causes localized injury with resulting scarring and fibrosis of the nerve. This leads to symptoms in the distribution of the nerve.
Symptoms
Patients with a Morton's neuroma typically experience a sharp, shooting or burning pain, usually at the base of the forefoot or toes, which radiates into the two affected toes. Sometimes the pain may also radiate into the foot. The pain is often associated with the presence of pins and needles and numbness.
Diagnosis
The physician will make the diagnosis of Morton's neuroma based upon the patient's symptoms as described above in an interview, or history, and a physical examination. The physical examination will reveal exceptional tenderness in the involved interspace when the nerve area is pressed on the bottom of the foot. As the interspace is palpated, and pressure is applied from the top to the bottom of the foot, a click can sometimes be felt which reproduces the patient's pain. This is known as a Mulder's sign. Because of inconsistent results, imaging studies such as MRI or ultrasound scanning are not useful diagnostic tools for Morton's neuroma. Thus the physician must rely exclusively on the patient's history and physical examination in order to make a diagnosis.
Non Surgical Treatment
You may be able to treat this problem at home. Avoid wearing tight, pointy, or high-heeled shoes. Choose well-fitted shoes with plenty of room for your toes. Put ice or a cold pack on the area for 10 to 15 minutes at a time. Put a thin cloth between the ice and your skin. Take anti-inflammatory medicines to reduce pain and swelling. These include ibuprofen (such as Advil or Motrin) and naproxen (such as Aleve). Rest your feet when you can. Reduce activities that put pressure on the toes, such as racquet sports or running. Try massaging your foot to relax the muscles around the nerve. If these steps do not relieve your symptoms, your doctor may have you use special pads or devices that spread the toes to keep them from squeezing the nerve. In some cases, a doctor may give a steroid shot to reduce swelling and pain. If these treatments do not help, your doctor may suggest surgery.
Surgical Treatment
Operative treatment of Morton?s neuroma should be entertained only after failure of nonoperative management. Standard operative treatment involves identifying the nerve and cutting (resecting) it proximal to the point where it is irritate/injured. This is usually done through an incision on the top (dorsal) aspect of the foot, although in rare instances, an incision on the sole (plantar) aspect of the foot maybe used. An incision on the sole of the foot works very well, unless an excessive scar forms in which case it can be problematic. Some physicians will attempt to treat Morton?s neuroma by releasing the intermetatarsal ligament and freeing the nerve of local scar tissue. This may also be beneficial.
Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.Causes
In many cases, a neuroma may develop as a result of excessive loading on the front of the foot. Sometimes, a patient?s anatomic alignment in the forefoot contributes to the overload. There may be some cases where the neuroma develops spontaneously, for no obvious reason. However, once the nerve is irritated, pressure from walking, and from the adjacent bony prominences (metatarsal heads), as well as from the intermetatarsal ligament that binds the heads together, all may contribute to persistent pain. Repetitive pressure on the nerve causes localized injury with resulting scarring and fibrosis of the nerve. This leads to symptoms in the distribution of the nerve.
Symptoms
Patients with a Morton's neuroma typically experience a sharp, shooting or burning pain, usually at the base of the forefoot or toes, which radiates into the two affected toes. Sometimes the pain may also radiate into the foot. The pain is often associated with the presence of pins and needles and numbness.
Diagnosis
The physician will make the diagnosis of Morton's neuroma based upon the patient's symptoms as described above in an interview, or history, and a physical examination. The physical examination will reveal exceptional tenderness in the involved interspace when the nerve area is pressed on the bottom of the foot. As the interspace is palpated, and pressure is applied from the top to the bottom of the foot, a click can sometimes be felt which reproduces the patient's pain. This is known as a Mulder's sign. Because of inconsistent results, imaging studies such as MRI or ultrasound scanning are not useful diagnostic tools for Morton's neuroma. Thus the physician must rely exclusively on the patient's history and physical examination in order to make a diagnosis.
Non Surgical Treatment
You may be able to treat this problem at home. Avoid wearing tight, pointy, or high-heeled shoes. Choose well-fitted shoes with plenty of room for your toes. Put ice or a cold pack on the area for 10 to 15 minutes at a time. Put a thin cloth between the ice and your skin. Take anti-inflammatory medicines to reduce pain and swelling. These include ibuprofen (such as Advil or Motrin) and naproxen (such as Aleve). Rest your feet when you can. Reduce activities that put pressure on the toes, such as racquet sports or running. Try massaging your foot to relax the muscles around the nerve. If these steps do not relieve your symptoms, your doctor may have you use special pads or devices that spread the toes to keep them from squeezing the nerve. In some cases, a doctor may give a steroid shot to reduce swelling and pain. If these treatments do not help, your doctor may suggest surgery.
Surgical Treatment
Operative treatment of Morton?s neuroma should be entertained only after failure of nonoperative management. Standard operative treatment involves identifying the nerve and cutting (resecting) it proximal to the point where it is irritate/injured. This is usually done through an incision on the top (dorsal) aspect of the foot, although in rare instances, an incision on the sole (plantar) aspect of the foot maybe used. An incision on the sole of the foot works very well, unless an excessive scar forms in which case it can be problematic. Some physicians will attempt to treat Morton?s neuroma by releasing the intermetatarsal ligament and freeing the nerve of local scar tissue. This may also be beneficial.
Treat Leg Length Difference With Shoe Lifts
There are actually two different kinds of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is anatomically shorter than the other. Through developmental stages of aging, the human brain picks up on the walking pattern and recognizes some variance. The entire body usually adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch isn't really excessive, does not need Shoe Lifts to compensate and normally won't have a serious effect over a lifetime.

Leg length inequality goes largely undiagnosed on a daily basis, yet this problem is simply remedied, and can eliminate a number of incidents of lumbar pain.
Therapy for leg length inequality usually involves Shoe Lifts. Most are very reasonably priced, commonly being under twenty dollars, compared to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Mid back pain is the most widespread condition afflicting people today. Over 80 million men and women are affected by back pain at some point in their life. It is a problem that costs businesses millions of dollars year after year due to lost time and output. Innovative and superior treatment methods are constantly sought after in the hope of reducing the economic influence this condition causes.

Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of reducing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous expert orthopaedic orthopedists.
In order to support the human body in a healthy and balanced fashion, feet have a critical part to play. Despite that, it is often the most overlooked region of the body. Some people have flat-feet which means there may be unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be impacted too. Shoe Lifts ensure that proper posture and balance are restored.
Leg length inequality goes largely undiagnosed on a daily basis, yet this problem is simply remedied, and can eliminate a number of incidents of lumbar pain.
Therapy for leg length inequality usually involves Shoe Lifts. Most are very reasonably priced, commonly being under twenty dollars, compared to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Mid back pain is the most widespread condition afflicting people today. Over 80 million men and women are affected by back pain at some point in their life. It is a problem that costs businesses millions of dollars year after year due to lost time and output. Innovative and superior treatment methods are constantly sought after in the hope of reducing the economic influence this condition causes.
Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of reducing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous expert orthopaedic orthopedists.
In order to support the human body in a healthy and balanced fashion, feet have a critical part to play. Despite that, it is often the most overlooked region of the body. Some people have flat-feet which means there may be unequal force placed on the feet. This will cause other body parts including knees, ankles and backs to be impacted too. Shoe Lifts ensure that proper posture and balance are restored.
What Is A Calcaneal Spur

Overview
The term heel spur generally refers more specifically to a heel spur, also known as a calcaneal spur. These calcium growths form around the tendons and ligaments of the foot and eventually become attached to the heel bone. The spurs then continue to grow, piercing the skin of the foot and causing pain and discomfort. When left untreated the spur can continue to grow causing agonizing pain and even immobilizing the patient.
Causes
One common cause of heel spurs and related injuries is due to abnormal mechanics and movement of the foot, also referred to as pronation. Abnormal gait, which is the way our feet hit the ground as we walk, also stresses the tissue of the foot, leading to conditions such as plantar fasciitis and heel spurs. Pronation can cause the foot to become unstable during movement, affecting the gait and leading to damage. A sudden increase in weight can also influence the development of a painful heel spur.
Symptoms
You'll typically first notice early heel spur pain under your heel in the morning or after resting. Your heel pain will be worse with the first steps and improves with activity as it warms up. When you palpate the tender area you may feel a tender bony lump. As your plantar fasciitis deteriorates and your heel spur grows, the pain will be present more often.
Diagnosis
Diagnosis of a heel spur can be done with an x-ray, which will be able to reveal the bony spur. Normally, it occurs where the plantar fascia connects to the heel bone. When the plantar fascia ligament is pulled excessively it begins to pull away from the heel bone. When this excessive pulling occurs, it causes the body to respond by depositing calcium in the injured area, resulting in the formation of the bone spur. The Plantar fascia ligament is a fibrous band of connective tissue running between the heel bone and the ball of the foot. This structure maintains the arch of the foot and distributes weight along the foot as we walk. However, due to the stress that this ligament must endure, it can easily become damaged which commonly occurs along with heel spurs.
Non Surgical Treatment
Diathermy treatment uses an electrical current to produce heat that sedates the inflamed tissues. The ultrasound device sends sound waves into the heel and sets up a massaging action that stimulates blood circulation. Treatment with a whirlpool bath involves placing the foot directly into the jetting stream. Orthopedic molds and appliances, such as orthotics, are designed by foot specialists for use inside the shoe to eliminate irritation to the heel when the patient stands or walks. When those appliances are used, the spur (in effect) floats on air. At the same time, the body's weight is transferred forward from the tender spot.
Surgical Treatment
Surgery to correct for heel spur syndrome is a common procedure which releases plantar fascia partially from its attachment to the calcaneous (heel bone). This part of the surgery is called a plantar fasciotomy due to the fact the fascia is cut. This is most often done through an open procedure as any heel spur or bursa can be removed at the same time. If the spur is not removed during the surgery, it will probably be just as successful, as the large spur is not the true problem. Some physicians use an endoscopic approach (EPF) where a small camera aids the physician during surgery with typically smaller incisions on each side of your foot.
Posterior Calcaneal Spur Treatment

Overview
The heel bone is the largest bone in the foot and absorbs the most shock and pressure. A heel spur develops as an abnormal growth of the heel bone. Most commonly, calcium deposits form when the plantar fascia pulls away from the heel area, causing a bony protrusion, or heel spur to develop. While bone spurs can develop in other locations such as the rear of the heel bone, this is the most common location for development. The plantar fascia is a broad band of fibrous tissue located along the bottom surface of the foot that runs from the heel to the forefoot. Heel spurs can cause extreme pain in the rearfoot, especially while standing or walking.
Causes
Heel spurs occur when calcium deposits build up on the underside of the heel bone, a process that usually occurs over a period of many months. Heel spurs are often caused by strains on foot muscles and ligaments, stretching of the plantar fascia, and repeated tearing of the membrane that covers the heel bone. Heel spurs are especially common among athletes whose activities include large amounts of running and jumping. Risk factors for heel spurs include walking gait abnormalities,which place excessive stress on the heel bone, ligaments, and nerves near the heel. Running or jogging, especially on hard surfaces. Poorly fitted or badly worn shoes, especially those lacking appropriate arch support. Excess weight and obesity. Other risk factors associated with plantar fasciitis include increasing age, which decreases plantar fascia flexibility and thins the heel's protective fat pad. Diabetes. Spending most of the day on one's feet. Frequent short bursts of physical activity. Having either flat feet or high arches.

Symptoms
Most heel spurs cause no symptoms and may go undetected for years. If they cause no pain or discomfort, they require no treatment. Occasionally, a bone spur will break off from the larger bone, becoming a ?loose body?, floating in a joint or embedding itself in the lining of the joint. This can cause pain and intermittent locking of the joint. In the case of heel spurs, sharp pain and discomfort is felt on the bottom of the foot or heel.
Diagnosis
Your doctor will discuss your medical history and will examine your foot and heel for any deformities and inflammation (swelling, redness, heat, pain). He/she will analyze your flexibility, stability, and gait (the way you walk). Occasionally an x-ray or blood tests (to rule out diseases or infections) may be requested.
Non Surgical Treatment
There are many ways to treat heel spurs. Some remedies you can even do at home once a podiatrist shows you how. Heel spur treatment is very similar to treatment of plantar fasciitis. Here are a few of the most common treatments. First, your doctor will assess which activities are causing your symptoms and suggest rest and time off from these activities. Ice packs are used to control pain and reduce symptoms. Certain exercises and stretches help you to feel relief quickly. Medications that reduce inflammation and decrease pain are also used. Sometimes cortisone injections are given. Often special shoe orthotics can help to take the pressure off of the plantar fascia and reduce symptoms. Night splints that keep your heel stretched are sometimes recommended. Rarely, surgery is an option. A new treatment called extracorporeal shock wave therapy is being studied.
Surgical Treatment
Usually, heel spurs are curable with conservative treatment. If not, heel spurs are curable with surgery, although there is the possibility of them growing back. About 10% of those who continue to see a physician for plantar fascitis have it for more than a year. If there is limited success after approximately one year of conservative treatment, patients are often advised to have surgery.
Prevention
If you have not yet developed this condition, you can take steps to protect yourself from it. Most importantly, make it a rule to wear properly fitted footwear. Avoid shoes that have become worn down in the heel, and don't choose shoes that cause you to walk in an abnormal fashion. Maintaining a healthy weight will ensure that undue pressure isn't being put on the ligaments, tendons and bones of your feet. If your job requires a great deal of time on your feet, or if you exercise regularly, be sure to balance periods of activity with periods of rest for your feet.