Bunion Splint Effectiveness
Overview
 If you have bunions, taking care of them now can help you avoid more serious treatment later. A bunion is a bump that forms on the joint of the big toe when bone or tissue moves out of place and extends beyond the normal anatomy of the toe. Left untreated, bunions can cause debilitating pain and may require surgery to correct.
If you have bunions, taking care of them now can help you avoid more serious treatment later. A bunion is a bump that forms on the joint of the big toe when bone or tissue moves out of place and extends beyond the normal anatomy of the toe. Left untreated, bunions can cause debilitating pain and may require surgery to correct.
Causes
Shoes. The primary cause of bunions is the long term use of shoes, particularly tight-fitting shoes with pointed toes, or high heeled shoes. A study that examined people in cultures that do not wear shoes found no cases of bunions. Genetic. People who have misaligned toes or feet, are flatfooted with feet that roll inwards (over pronation), excessive flexibility of ligaments, abnormal bone structure, or have mechanical instability in the big toe joint are more susceptible to bunions. This is especially common when bunions occur in children or young adults. Injuries or other trauma (sprains, fractures or nerve injuries), neuromuscular disorders (polio or Charcot-Marie-Tooth disease), or limb-length discrepancies (one leg longer than the other). Repetitive stresses to the foot. Bunions are common in ballet dancers and in a few sports. Arthritis.
Symptoms
Signs and symptoms of a bunion include the base of the big toe is swollen and sticks out. The big toe is often bent towards the other toes, and sometimes the second toe is pushed to overlap the third toe. Skin around the big toe joint is red and sore. Thickened skin at the base of the big toe. Pain in the big toe or foot. Wearing shoes is painful. Pain or difficulty when walking.
Diagnosis
Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly.
Non Surgical Treatment
Bunions can be treated conservatively (without surgery) using simple measures such as well-fitting shoes, orthoses simple painkillers and padding. Physiotherapy can help improve associated muscle imbalances. Such measures will not correct or even stop the deformity but they can help with symptoms. When non-surgical treatments prove insufficient, surgery can relieve your pain, correct any related foot deformity and help you resume your normal activities. 
Surgical Treatment
For those whose bunions cause persisting pain, a surgical operation is considered for correction of the bunion. The surgical operation to correct a bunion is referred to as a bunionectomy. Surgical procedures can correct deformity and relieve pain, leading to improved foot function. These procedures typically involve removing bony growth of the bunion while realigning the big toe joint. Surgery is often, but not always, successful; failure to relieve pain can result from the big toe moving back to its previous deviated position even after surgery. However, proper footwear and orthotics can reduce the chances of surgical failure.
Find Out About Overpronation Of The Foot
Overview
Overpronation is the most common abnormality found in the foot, and for this reason, is the most studied. The term that most people attribute to overpronation is ?flat feet.? Pronation is the rolling in of the foot and the collapse of the arch. Every person pronates to some extent and this is a necessary moment in the normal walking cycle as it allows the forefoot to make complete contact with the ground. A foot that overpronates acts like a loose bag of bones during the walking cycle. This makes this type of foot very flexible but inefficient. The foot has to work much harder to propel the body, fatiguing easily and placing mechanical stresses on the lower body. We like to use the analogy of digging a hole in the dirt. Overpronating feet are like using a broom to dig the hole. It won?t break down quickly, but you will be digging for a very long time, or until eventually wear and tear will take effect. Wouldn?t you rather have a shovel to work with. This is in essence what an orthotic can do for your feet. This is why orthotics have become an evidence based treatment for so many foot ailments, as they can effectively manage overpronation.Overpronation is when a person pronates too much and for too long. This places excess stress on the tendons and ligaments in the foot and ankle.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Not all foot injuries affecting runners are necessarily down to a particular running gait; it is rarely that simple to diagnose how a foot problem developed . Simply being an overpronator does not mean that a foot injury has been caused by the running gait and it could be due to a number of factors. However mild to severe overpronators tend to be at a higher risk of developing musculoskeletal problems due to the increased stresses and strains which are placed on the body when the foot does not move in an optimum manner. The following injuries are frequently due to overpronation of the feet. Tarsal tunnel syndrome. Shin splints. Anterior compartment syndrome. Plantar fasciitis. Achilles tendonitis. Bunions. Sesamoiditis. Stress fractures. Back and hip pain. Ankle pain.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Your podiatrist will look at your current footwear to ensure that it is both well-fitted and possessed of adequate cushioning to protect your feet. Firm heel support is advised for over-pronators, and a good fit is important to ensure that the foot as a whole is well supported as instability can exacerbate the existing problems caused by over-pronation.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Overpronation is the most common abnormality found in the foot, and for this reason, is the most studied. The term that most people attribute to overpronation is ?flat feet.? Pronation is the rolling in of the foot and the collapse of the arch. Every person pronates to some extent and this is a necessary moment in the normal walking cycle as it allows the forefoot to make complete contact with the ground. A foot that overpronates acts like a loose bag of bones during the walking cycle. This makes this type of foot very flexible but inefficient. The foot has to work much harder to propel the body, fatiguing easily and placing mechanical stresses on the lower body. We like to use the analogy of digging a hole in the dirt. Overpronating feet are like using a broom to dig the hole. It won?t break down quickly, but you will be digging for a very long time, or until eventually wear and tear will take effect. Wouldn?t you rather have a shovel to work with. This is in essence what an orthotic can do for your feet. This is why orthotics have become an evidence based treatment for so many foot ailments, as they can effectively manage overpronation.Overpronation is when a person pronates too much and for too long. This places excess stress on the tendons and ligaments in the foot and ankle.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Not all foot injuries affecting runners are necessarily down to a particular running gait; it is rarely that simple to diagnose how a foot problem developed . Simply being an overpronator does not mean that a foot injury has been caused by the running gait and it could be due to a number of factors. However mild to severe overpronators tend to be at a higher risk of developing musculoskeletal problems due to the increased stresses and strains which are placed on the body when the foot does not move in an optimum manner. The following injuries are frequently due to overpronation of the feet. Tarsal tunnel syndrome. Shin splints. Anterior compartment syndrome. Plantar fasciitis. Achilles tendonitis. Bunions. Sesamoiditis. Stress fractures. Back and hip pain. Ankle pain.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Your podiatrist will look at your current footwear to ensure that it is both well-fitted and possessed of adequate cushioning to protect your feet. Firm heel support is advised for over-pronators, and a good fit is important to ensure that the foot as a whole is well supported as instability can exacerbate the existing problems caused by over-pronation.
Prevention
Firstly, a thorough and correct warm up will help to prepare the muscles and tendons for any activity or sport. Without a proper warm up the muscles and tendons around your feet, ankles and lower legs will be tight and stiff. There will be limited blood flow to the lower legs, which will result in a lack of oxygen and nutrients for those muscles. Click here for a detailed explanation of how, why and when to perform your warm up. Secondly, flexible muscles are extremely important in the prevention of most ankle and lower leg injuries. When muscles and tendons are flexible and supple, they are able to move and perform without being over stretched. If however, your muscles and tendons are tight and stiff, it is quite easy for those muscles and tendons to be pushed beyond their natural range of motion. To keep your muscles and tendons flexible and supple, it is important to undertake a structured stretching routine.
Can One Take Care Of Severs Disease In The Home?
Overview
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
The foot is one of the first body parts to grow to full size. During the time of growth, bones grow faster than muscles and tendons. This results in the muscles and tendons becoming tight. The strongest tendon that attaches to the heel is the Achilles Tendon. It attaches to the back of the heel at the site of the growth plate, and during sports activities it pulls with great force on the growth plate. If this pull by the tight Achilles Tendon (calf muscle) continues for long periods of time, the growth plate may become inflamed and painful. If exertive activities continue, Sever's Disease may result.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Ice the heel(s) well after exercise (until the area is cold and numb!) Stretch hamstring and calf muscles 2-3 times daily (exercises below) REST when pain becomes persistent or moderate (even if it means skipping games or practices.) Anti-inflammatory medication such as ibuprofen. If symptoms persist, your child may need to see a physical therapist for additional exercises, and/or an orthopedist for othotics or temporary casting/crutches if pain is severe. Sever?s disease is self-recovering, meaning that it will go away on its own when the heels are rested or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. However, pain can recur, for example at the start of a new sports season, several times if it is not taken care of.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
Severs disease or calcaneal apophysitis causes heel pain usually in growing children between age nine and fourteen. It occurs as a result of disturbance during the final development of the heel growth plate. During this time the achilles tendon is pulling strongly on the heel bone and this excessive force can cause inflammation and pain.
Causes
The foot is one of the first body parts to grow to full size. During the time of growth, bones grow faster than muscles and tendons. This results in the muscles and tendons becoming tight. The strongest tendon that attaches to the heel is the Achilles Tendon. It attaches to the back of the heel at the site of the growth plate, and during sports activities it pulls with great force on the growth plate. If this pull by the tight Achilles Tendon (calf muscle) continues for long periods of time, the growth plate may become inflamed and painful. If exertive activities continue, Sever's Disease may result.
Symptoms
Sever?s disease is a clinical diagnosis based on the youth?s presenting symptoms, rather than on diagnostic tests. While x-rays may be ordered in the process of diagnosing the disease, they are used primarily to rule out bone fractures or other bone abnormalities, rather than to confirm the disease. Common Characteristics of Sever?s Disease include Posterior inferior heel pain. Pain is usually absent when waking in the morning. Increased pain with weight bearing, running, or jumping (or activity-related pain). Area often feels stiff or inflexible. Youth may limp at the end of physical activity. Tenderness at the insertion of the tendons. Limited ankle dorsiflexion range that is secondary to tightness of the Achilles tendon. Activity or sport practices on hard surfaces can also contribute to pain, as well as poor quality shoes, worn out shoes, or the wrong shoes for the sport. Typically, the pain from this disease gradually resolves with rest.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
Ice the heel(s) well after exercise (until the area is cold and numb!) Stretch hamstring and calf muscles 2-3 times daily (exercises below) REST when pain becomes persistent or moderate (even if it means skipping games or practices.) Anti-inflammatory medication such as ibuprofen. If symptoms persist, your child may need to see a physical therapist for additional exercises, and/or an orthopedist for othotics or temporary casting/crutches if pain is severe. Sever?s disease is self-recovering, meaning that it will go away on its own when the heels are rested or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. However, pain can recur, for example at the start of a new sports season, several times if it is not taken care of.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
Posterior Tibial Tendon Dysfunction Surgery Prognosis
Overview
Have you noticed that the medial arch of your foot is becoming flatter when you walk? You may be developing adult acquired flat foot. This condition is typically caused by a problem with a tendon on the medial side of your foot called the Posterior Tibial Tendon that is not functioning well. You may experience pain in the inner side of your foot when you walk. The affected foot appears to roll outwards (the sole of the foot is trying to face outwards) when you walk. This is called over-pronation of the foot. The back of your heel may start to point outwards (heel valgus). Over time you may lose the ability to tip toe on that foot as the posterior tibial tendon stretches out and it may eventually tear. 
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder.
Symptoms
Most people will notice mild to extreme pain in their feet. Below outlines some signs and symptoms of AAFD. Trouble walking or standing for any duration. Pain and swelling on the inside of the ankle. Bump on the bottom of the foot. Ulcer or wound developing on the outer aspects of foot.
Diagnosis
Observe forefoot to hindfoot alignment. Do this with the patient sitting and the heel in neutral, and also with the patient standing. I like to put blocks under the forefoot with the heel in neutral to see how much forefoot correction is necessary to help hold the hindfoot position. One last note is to check all joints for stiffness. In cases of prolonged PTTD or coalition, rigid deformity is present and one must carefully check the joints of the midfoot and hindfoot for stiffness and arthritis in the surgical pre-planning.
Non surgical Treatment
Conservative (nonoperative) care is advised at first. A simple modification to your shoe may be all that???s needed. Sometimes purchasing shoes with a good arch support is sufficient. For other patients, an off-the-shelf (prefabricated) shoe insert works well. The orthotic is designed specifically to position your foot in good alignment. Like the shoe insert, the orthotic fits inside the shoe. These work well for mild deformity or symptoms. Over-the-counter pain relievers or antiinflammatory drugs such as ibuprofen may be helpful. If symptoms are very severe, a removable boot or cast may be used to rest, support, and stabilize the foot and ankle while still allowing function. Patients with longer duration of symptoms or greater deformity may need a customized brace. The brace provides support and limits ankle motion. After several months, the brace is replaced with a foot orthotic. A physical therapy program of exercise to stretch and strengthen the foot and leg muscles is important. The therapist will also show you how to improve motor control and proprioception (joint sense of position). These added features help prevent and reduce injuries. 
Surgical Treatment
Although non-surgical treatments can successfully manage the symptoms, they do not correct the underlying problem. It can require a life-long commitment to wearing the brace during periods of increased pain or activity demands. This will lead a majority of patients to choose surgical correction of the deformity, through Reconstructive Surgery. All of the considerations that were extremely important during the evaluation stage become even more important when creating a surgical plan. Generally, a combination of procedures are utilized in the same setting, to allow full correction of the deformity. Many times, this can be performed as a same-day surgery, without need for an overnight hospital stay. However, one or two day hospital admissions can be utilized to help manage the post-operative pain. Although the recovery process can require a significant investment of time, the subsequent decades of improved function and activity level, as well as decreased pain, leads to a substantial return on your investment.
Heel Serious Pain Everything You Should Know Heel Ache
Overview

The most common form of Heel Pain, is pain on the bottom of the heel. It tends to occur for no apparent reason and is often worse when first placing weight on the foot. Patients often complain of pain the first thing in the morning or after getting up to stand after sitting. The pain can be a sharp, searing pain or present as a tearing feeling in the bottom of the heel. As the condition progresses there may be a throbbing pain after getting off your feet or there may be soreness that radiates up the back of the leg. Pain may also radiate into the arch of the foot.
Causes
Heel pain can have many causes. If your heel hurts, see your primary care doctor or orthopaedic foot and ankle specialist right away to determine why and get treatment. Tell him or her exactly where you have pain and how long you've had it. Your doctor will examine your heel, looking and feeling for signs of tenderness and swelling. You may be asked to walk, stand on one foot or do other physical tests that help your doctor pinpoint the cause of your sore heel. Conditions that cause heel pain generally fall into two main categories: pain beneath the heel and pain behind the heel.
Symptoms
See your doctor immediately if you have Severe pain and swelling near your heel. Inability to bend your foot downward, rise on your toes or walk normally. Heel pain with fever, numbness or tingling in your heel. Severe heel pain immediately after an injury. Schedule an office visit if you have. Heel pain that continues when you're not walking or standing. Heel pain that lasts more than a few weeks, even after you've tried rest, ice and other home treatments.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Most heel pain is caused by a combination of poor biomechanics, or muscle weakness or tightness. The good news is that heel pain can be effectively managed once the cause is identified. Most heel pain can be successfully treated via pain and pressure relief techniques, biomechanical correction eg orthotics, taping, foot posture exercises, muscle stretches and massage, lower limb muscle strengthening, proprioceptive and balance exercises to stimulate your foot intrinsic muscles. If you feel that your footwear or sports training schedule are potentially causing your heel pain, then we recommend that you seek the advice of a sports physiotherapist, podiatrist or trained footwear specialist (not just a shop assistant) to see if your shoe is a match for your foot; or discuss your training regime to see if you are doing too much. Heel pain and injury are extremely common. With accurate assessment and early treatment most heel pain injuries respond extremely quickly to physiotherapy allowing you to quickly resume pain-free and normal activities of daily living. Please ask you physiotherapist for their professional treatment advice.
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention
You can help to prevent heel pain by maintaining a healthy weight, by warming up before participating in sports and by wearing shoes that support the arch of the foot and cushion the heel. If you are prone to plantar fasciitis, exercises that stretch the Achilles tendon (heel cord) and plantar fascia may help to prevent the area from being injured again. You also can massage the soles of your feet with ice after stressful athletic activities. Sometimes, the only interventions needed are a brief period of rest and new walking or running shoes.
The most common form of Heel Pain, is pain on the bottom of the heel. It tends to occur for no apparent reason and is often worse when first placing weight on the foot. Patients often complain of pain the first thing in the morning or after getting up to stand after sitting. The pain can be a sharp, searing pain or present as a tearing feeling in the bottom of the heel. As the condition progresses there may be a throbbing pain after getting off your feet or there may be soreness that radiates up the back of the leg. Pain may also radiate into the arch of the foot.
Causes
Heel pain can have many causes. If your heel hurts, see your primary care doctor or orthopaedic foot and ankle specialist right away to determine why and get treatment. Tell him or her exactly where you have pain and how long you've had it. Your doctor will examine your heel, looking and feeling for signs of tenderness and swelling. You may be asked to walk, stand on one foot or do other physical tests that help your doctor pinpoint the cause of your sore heel. Conditions that cause heel pain generally fall into two main categories: pain beneath the heel and pain behind the heel.
Symptoms
See your doctor immediately if you have Severe pain and swelling near your heel. Inability to bend your foot downward, rise on your toes or walk normally. Heel pain with fever, numbness or tingling in your heel. Severe heel pain immediately after an injury. Schedule an office visit if you have. Heel pain that continues when you're not walking or standing. Heel pain that lasts more than a few weeks, even after you've tried rest, ice and other home treatments.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Most heel pain is caused by a combination of poor biomechanics, or muscle weakness or tightness. The good news is that heel pain can be effectively managed once the cause is identified. Most heel pain can be successfully treated via pain and pressure relief techniques, biomechanical correction eg orthotics, taping, foot posture exercises, muscle stretches and massage, lower limb muscle strengthening, proprioceptive and balance exercises to stimulate your foot intrinsic muscles. If you feel that your footwear or sports training schedule are potentially causing your heel pain, then we recommend that you seek the advice of a sports physiotherapist, podiatrist or trained footwear specialist (not just a shop assistant) to see if your shoe is a match for your foot; or discuss your training regime to see if you are doing too much. Heel pain and injury are extremely common. With accurate assessment and early treatment most heel pain injuries respond extremely quickly to physiotherapy allowing you to quickly resume pain-free and normal activities of daily living. Please ask you physiotherapist for their professional treatment advice.
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention
You can help to prevent heel pain by maintaining a healthy weight, by warming up before participating in sports and by wearing shoes that support the arch of the foot and cushion the heel. If you are prone to plantar fasciitis, exercises that stretch the Achilles tendon (heel cord) and plantar fascia may help to prevent the area from being injured again. You also can massage the soles of your feet with ice after stressful athletic activities. Sometimes, the only interventions needed are a brief period of rest and new walking or running shoes.
Precisely What Will Cause Tendinitis Pain Of The Achilles ?
Overview
 The Achilles tendon is the largest and strongest tendon in the human body. It is the ?cord? in the back of the leg that inserts into the back of the heel. The Achilles tendon got its name, according to Greek legend, when the Greek warrior, Achilles, was dipped into the River Styx by Thetis, his mother. This rendered him invincible with the exception of his unsubmerged heel. Unfortunately, he went on to get mortally wounded during the siege of Troy when he was struck in that heel by an arrow. Achilles tendinitis is inflammation and partial tearing of the Achilles tendon. It can occur with overuse of the tendon such as when starting or increasing the intensity of an exercise program or performing impact loading activities that include a lot of running and/or jumping.
The Achilles tendon is the largest and strongest tendon in the human body. It is the ?cord? in the back of the leg that inserts into the back of the heel. The Achilles tendon got its name, according to Greek legend, when the Greek warrior, Achilles, was dipped into the River Styx by Thetis, his mother. This rendered him invincible with the exception of his unsubmerged heel. Unfortunately, he went on to get mortally wounded during the siege of Troy when he was struck in that heel by an arrow. Achilles tendinitis is inflammation and partial tearing of the Achilles tendon. It can occur with overuse of the tendon such as when starting or increasing the intensity of an exercise program or performing impact loading activities that include a lot of running and/or jumping.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
Pain anywhere along the tendon, but most often on or close to the heel. Swelling of the skin over the tendon, associated with warmth, redness and tenderness. Pain on rising up on the toes and pain with pushing off on the toes. If you are unable to stand on your toes you may have ruptured the tendon. This requires urgent medical attention. A painful heel for the first few minutes of walking after waking up in the morning. Stiffness of the ankle, which often improves with mild activity.
Diagnosis
Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Imaging studies. Plain radiography: Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography: Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst; in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI): MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis.
Nonsurgical Treatment
Wear shoes with a low half-inch to one-inch heel that are somewhat flexible through the ball of the foot. Avoid flat footwear such as slippers or sandals and stiff shoes. Add a heel lift in your shoe. You may also use arch support inserts or orthotic insoles. Heel lifts and orthotics can be purchased at many of our pharmacies and Podiatry departments. Avoid standing or walking barefoot. Perform calf-stretching exercises for 30 to 60 seconds on each leg at least 2 times a day. Stand an arm?s length away from a wall, facing the wall. Lean into the wall, stepping forward with one leg, leaving the other stretched behind you. The leg behind you is the one being stretched. Keep this leg straight (locked) and the toes pointed straight at the wall. Stretch forward until you feel tightness in the calf of your back leg. Hold this position without bouncing for 30 to 60 seconds. Repeat for the opposite leg. Do stair exercises every day. Stand facing the stairs with the ball of your foot on a stair and your heel hanging off. Balance on one foot at a time while holding onto the rail. Slowly lower your heel as low as it will drop down and then slowly raise it up as high as you can lift it. Repeat this exercise slowly several times on each foot. Perform this exercise every other day, gradually increasing the number of repetitions over time as tolerated. If you are overweight, talk to your personal physician about resources that can help you lose weight. Carrying excess weight places additional pressure on your feet. Decrease the time that you stand, walk, or engage in exercises that put a load on your feet. Switch to a nonimpact form of exercise until your tendon heals, such as swimming, pool running, and using an elliptical trainer.

Surgical Treatment
Treating this surgically, there are numerous methods to repair the tendon. Most commonly, Achilles tendon is exposed through an incision at the back of the ankle. After identifying both ends of ruptured tendon, the edges got trimmed and then both ends were sutured together with optimal tension. To get a better outcome with fixation, an anchor may have to be in place in calcaneus, provided the rupture is very low. Care must be taken to avoid injuries to the nerves located adjacent to the tendon.
Prevention
Appropriately warm up and stretch before practice or competition. Allow time for adequate rest and recovery between practices and competition. Maintain appropriate conditioning, Ankle and leg flexibility, Muscle strength and endurance, Cardiovascular fitness. Use proper technique. To help prevent recurrence, taping, protective strapping, or an adhesive bandage may be recommended for several weeks after healing is complete.
The Achilles tendon is the largest and strongest tendon in the human body. It is the ?cord? in the back of the leg that inserts into the back of the heel. The Achilles tendon got its name, according to Greek legend, when the Greek warrior, Achilles, was dipped into the River Styx by Thetis, his mother. This rendered him invincible with the exception of his unsubmerged heel. Unfortunately, he went on to get mortally wounded during the siege of Troy when he was struck in that heel by an arrow. Achilles tendinitis is inflammation and partial tearing of the Achilles tendon. It can occur with overuse of the tendon such as when starting or increasing the intensity of an exercise program or performing impact loading activities that include a lot of running and/or jumping.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
Pain anywhere along the tendon, but most often on or close to the heel. Swelling of the skin over the tendon, associated with warmth, redness and tenderness. Pain on rising up on the toes and pain with pushing off on the toes. If you are unable to stand on your toes you may have ruptured the tendon. This requires urgent medical attention. A painful heel for the first few minutes of walking after waking up in the morning. Stiffness of the ankle, which often improves with mild activity.
Diagnosis
Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Imaging studies. Plain radiography: Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography: Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst; in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI): MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis.
Nonsurgical Treatment
Wear shoes with a low half-inch to one-inch heel that are somewhat flexible through the ball of the foot. Avoid flat footwear such as slippers or sandals and stiff shoes. Add a heel lift in your shoe. You may also use arch support inserts or orthotic insoles. Heel lifts and orthotics can be purchased at many of our pharmacies and Podiatry departments. Avoid standing or walking barefoot. Perform calf-stretching exercises for 30 to 60 seconds on each leg at least 2 times a day. Stand an arm?s length away from a wall, facing the wall. Lean into the wall, stepping forward with one leg, leaving the other stretched behind you. The leg behind you is the one being stretched. Keep this leg straight (locked) and the toes pointed straight at the wall. Stretch forward until you feel tightness in the calf of your back leg. Hold this position without bouncing for 30 to 60 seconds. Repeat for the opposite leg. Do stair exercises every day. Stand facing the stairs with the ball of your foot on a stair and your heel hanging off. Balance on one foot at a time while holding onto the rail. Slowly lower your heel as low as it will drop down and then slowly raise it up as high as you can lift it. Repeat this exercise slowly several times on each foot. Perform this exercise every other day, gradually increasing the number of repetitions over time as tolerated. If you are overweight, talk to your personal physician about resources that can help you lose weight. Carrying excess weight places additional pressure on your feet. Decrease the time that you stand, walk, or engage in exercises that put a load on your feet. Switch to a nonimpact form of exercise until your tendon heals, such as swimming, pool running, and using an elliptical trainer.
Surgical Treatment
Treating this surgically, there are numerous methods to repair the tendon. Most commonly, Achilles tendon is exposed through an incision at the back of the ankle. After identifying both ends of ruptured tendon, the edges got trimmed and then both ends were sutured together with optimal tension. To get a better outcome with fixation, an anchor may have to be in place in calcaneus, provided the rupture is very low. Care must be taken to avoid injuries to the nerves located adjacent to the tendon.
Prevention
Appropriately warm up and stretch before practice or competition. Allow time for adequate rest and recovery between practices and competition. Maintain appropriate conditioning, Ankle and leg flexibility, Muscle strength and endurance, Cardiovascular fitness. Use proper technique. To help prevent recurrence, taping, protective strapping, or an adhesive bandage may be recommended for several weeks after healing is complete.
What Leads To Heel Pain And The Ways To Eliminate It

Overview
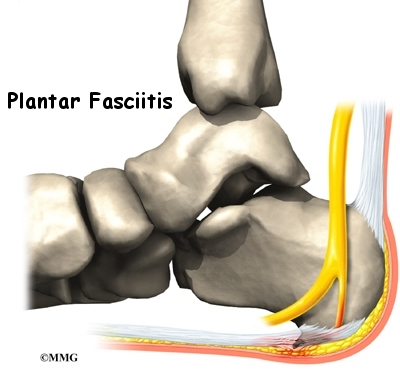
Plantar fasciitis is a common cause of heel pain in adults. The disorder classically presents with pain that is particularly severe with the first few steps taken in the morning. In general, plantar fasciitis is a self-limited condition. However, symptoms usually resolve more quickly when the interval between the onset of symptoms and the onset of treatment is shorter. Many treatment options exist, including rest, stretching, strengthening, change of shoes, arch supports, orthotics, night splints, anti-inflammatory agents and surgery. Usually, plantar fasciitis can be treated successfully by tailoring treatment to an individual's risk factors and preferences.
Causes
Identified risk factors for plantar fasciitis include excessive running, standing on hard surfaces for prolonged periods of time, high arches of the feet, the presence of a leg length inequality, and flat feet. The tendency of flat feet to excessively roll inward during walking or running makes them more susceptible to plantar fasciitis. Obesity is seen in 70% of individuals who present with plantar fasciitis and is an independent risk factor. Studies have suggested a strong association exists between an increased body mass index and the development of plantar fasciitis. Achilles tendon tightness and inappropriate footwear have also been identified as significant risk factors.
Symptoms
The most common symptom is pain and stiffness in the bottom of the heel. The heel pain may be dull or sharp. The bottom of the foot may also ache or burn. The pain is often worse in the morning when you take your first steps, after standing or sitting for awhile, when climbing stairs, after intense activity. The pain may develop slowly over time, or come on suddenly after intense activity.
Diagnosis
Your doctor may look at your feet and watch the way you stand, walk and exercise. He can also ask you questions about your health history, including illnesses and injuries that you had in your past. The symptoms you have such as the pain location or when does your foot hurts most. Your activity routine such as your job, exercise habits and physical activities preformed. Your doctor may decide to use an X-ray of your foot to detect bones problems. MRI or ultrasound can also be used as further investigation of the foot condition.
Non Surgical Treatment
Sometimes physical therapy modalities are helpful. The most frequently used modalities include ultrasound (high frequency sound vibrations that create a deep heat and reduce inflammation) and galvanic electrical stimulation ( a carefully applied intermittent muscular stimulation to the heel and calf that helps reduce pain and relax muscle spasm, which is a contributing factor to the pain). This treatment has been found most effective when given twice a week. Repeated taping and padding is sometimes used. The felt pads that will be strapped to your feet will compress after a few days and must be reapplied. While wearing them they should be kept dry, but may be removed the night before your next appointment. Resistant cases of heel pain caused by plantar fasciitis, heel spurs or cases of stress fracture of the calcaneus often need to be placed in a removable below knee cast boot. It is important to be aware of how your foot feels over this time period. If your foot is still uncomfortable without the strapping, but was more comfortable while wearing it, that is an indication that the treatment should help. Remember, what took many months or years to develop can not be eliminated in just a few days.

Surgical Treatment
The most common surgical procedure for plantar fasciitis is plantar fascia release. It involves surgical removal of a part from the plantar fascia ligament which will relieve the inflammation and reduce the tension. Plantar fascia release is either an open surgery or endoscopic surgery (insertion of special surgical instruments through small incisions). While both methods are performed under local anesthesia the open procedure may take more time to recover. Other surgical procedures can be used as well but they are rarely an option. Complications of plantar fasciitis surgery are rare but they are not impossible. All types of plantar fasciitis surgery pose a risk of infection, nerve damage, and anesthesia related complications including systemic toxicity, and persistence or worsening of heel pain.
Prevention
Stretching the plantar fascia and the calf muscle area can help to prevent inflammation. Slowly increasing the amount or intensity of athletic activities by graded progression can also help to prevent injury. Recommended Stretches: Taking a lunge position with the injured foot behind and keeping your heels flat on the floor, lean into a wall and bend the knees. A stretch should be felt in the sole and in the Achilles tendon area. Hold the stretch for 20-30 seconds. Also try this stretch with the back leg straight.